Courtesy: Prof Nabile Ebraheim,University of Toledo, Ohio, USA
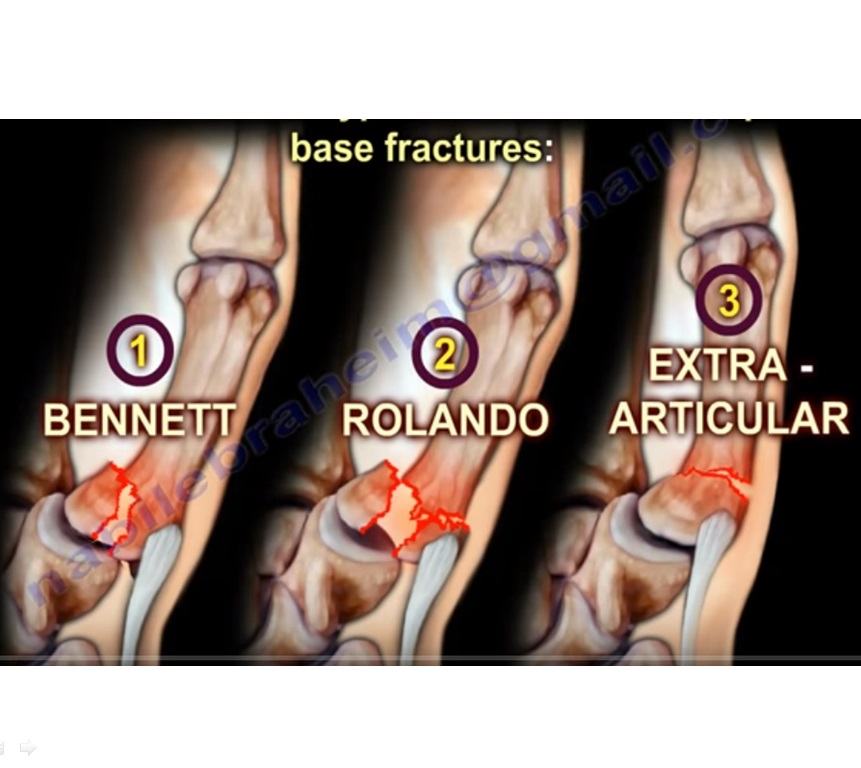
Fracture of the base of thumb metacarpal
The three types under it are the following:
1. Bennett fracture
2. Rolando’s fracture
3. Extra-articular fracture
Anatomy:
- There are five metacarpal bones in the hand.
- The first metacarpal bone is connected at the base to the trapezium at the first carpometacarpal joint.
- The carpometacarpal joint is a saddle shaped joint.
- The articulation between the first metacarpal bone and the trapezium gives inherent stability.
- Trapezium has a concave articular surface and the first metacarpal has a convex articular surface.
- Movement at the base of the thumb occurs around 2 axes:-
1. Flexion and extension
2. Abduction and adduction
And rotation. Counting fingers with the thumb is called opposition.
Muscle insertions :
1. Abductor pollicis longus (inserted at the base of the first metacarpal)
2. Adductor pollicis (inserted at the base of the proximal phalanx)
Bennett fracture
- It is a fracture dislocation at the base of the first metacarpal that extends into the carpometacarpal joint articulation.
- There is volar-ulnar beak fracture fragment
- Mechanism of injury:
Axial overload along the 1st metacarpal with simultaneous flexion (as in the case of fist fight)
Deformity:
1. The distal part of the first metacarpal is adducted by the adductor pollicis muscle (ulnar nerve supply).
2. The metacarpal head is displaced into the palm.
3. The metacarpal shaft is displaced proximally by the abductor pollicis longus muscle (posterior interosseous nerve supply)
4. The metacarpal is therefore displaced dorsally, radially and supinated.
5. The small volar lip ulnar fragment remains in its position attached to the trapezium by the oblique ligament.
6. The main deforming forces are the abductor pollicis longus and adductor pollicis muscles.
Investigation:
X-ray plain or Robert view (hyperpronated AP thumb ) and true lateral view
Treatment:
- Closed reduction percutaneous pinning or open reduction internal fixation if the fragment is large enough (more than 20%)
- Reducing the 1st metacarpal to restore the articular surface: give longitudinal traction.
- Pronate the metacarpal.
- Then apply pressure over the thumb base to push it back to its base by abduction and extension of the metacarpal
- The pinning will go from the thumb to the trapezium or from the thumb to the second metacarpal. Pinning may also go to both.
- Apply thumb spica splint
- Upto 2mm of articulation incongruity is accepted.
Note: The sensory branches of the radial nerve, radial artery and multiple tendons are in this area. Therefore the surgeon should be careful not to injure these structures during the surgery.
Reverse Bennett fracture
- Intra-articular fracture of the base of the fifth metacarpal bone which extends into the carpometacarpal joint. The extensor carpi ulnaris has a pulling action on the 5th metacarpal.
Rolando fracture
- Intra-articular, comminuted fracture through the base of the 1st metacarpal bone with same deforming forces as the Bennett fracture.
- The base of the 1st metacarpal is split onto volar and dorsal fragments.
- ‘Y’ fracture or transverse fracture
- Sometimes three or more intra-articular fragments are present.
Treatment:
- Difficult and controversial. Can be ORIF. Or closed reduction percutaneous pinning or external fixation.
- Prognosis is worse than Bennett fracture and may end in arthritis.
- Majority of cases do well even with residual displacement or incongruity.
Extra-articular fracture
- It has the best outcome
- Upto 30 degrees angulation is tolerated well. It can be managed with thumb spica splint
- Angulation more than 30 degrees may lead to MCP hyperextension.
- Therefore reduction and closed pinning is done. But in the case of high demand athletes, ORIF is done
Interesting article…thanks…
Very informative npractical thanq
many tnx