Courtesy: Prof Nabil Ebraheim
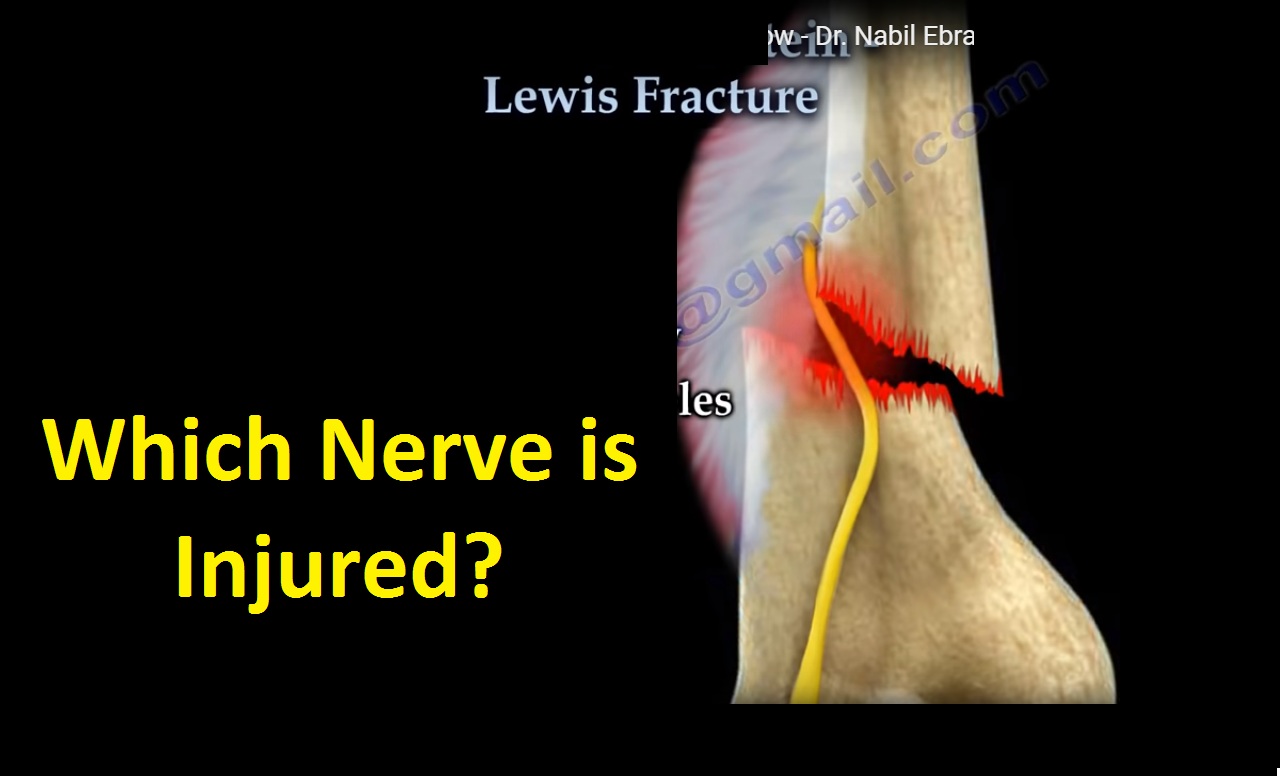
Holstein – Lewis fracture is a spiral fracture involving the distal third of the humerus, which causes entrapment of the radial nerve.The radial nerve originates from the posterior cord of the brachial plexus. As the radial nerve travels to the humerus, it provides innervation to the dorsal upper arm muscles.The radial nerve then travels anterior to give innervation to the extensor muscles of the wrist and hand.Interruption of the radial nerve such as with Holstein – Lewis fracture, will cause “wrist drop”. Radial nerve injury occurs in about 18% of cases involving fracture of the humerus.
Radial nerve injury is common with distal third fractures of the humerus, especially if the fragment is displaced laterally. As the nerve passes through the inter-muscular septum, it becomes trapped or lacerated.
The injuries to the nerve includes:
• Neuropraxia:
– Minor compression or contusion of the nerve.
– Similar to a temporary concussion.
• Axonotmesis:
– Injury causes a break down of the axon.
– The Schwann cell and endoneurium are left intact.
With temporary concussion of the nerve, 90% of injuries usually recover within 3-4 months.
If the fracture is open and associated with nerve injury, the nerve could be lacerated and exploration should be done.
Treatment:
– Open fracture: if open associated with radial nerve injury:
• Debride the wound.
• Exploration of the nerve and fixation of the fracture should be done.
The approach is anterolateral.
• Explore the nerve between the brachialis and the brachioradialis.
Posterior approach:
• Biomechanically better.
• The humerus is flat posteriorly, easy to apply the plate.
• Nerve exploration may be difficult.
Closed fracture:
• The fracture is treated usually without surgery according to the principles of fracture treatment.
• Observe the nerve for recovery.
Radial nerve palsy is not contraindicated of functional bracing.
Start obtaining EMG at 3-4 weeks.
Wrist extension is expected to recover before finger extension.
The brachioradialis muscle is the first to recover.
Positive sharp P-waves are Bad, Indication of acute denervation.
Polyphasic waves are Good, Polyphasic motor unit activity is early evidence of nerve regeneration.
The nerve can be explored after 4 months of observation if no recovery occurs with anticipation of nerve repair, nerve graft, or tendon transfer.
Sometimes working on the nerve in addition to tendon transfer is needed especially in younger patients.
Secondary injury from manipulation of the fracture may occur.
If injury occurs during manipulation of the fracture, a surgical option or nonsurgical option is open to debate.
Advantages of the late exploration:
– With late nerve exploration, the fracture may already be healing.
– The result of nerve repair is as good as primary exploration and repair
Leave a Reply