Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Lisfranc injuries are important and can be missed. Requires a high index of suspicion for its diagnosis. Lisfranc injuries can lead to an altered gait, midfoot arthritis and long-term disability.
Anatomy
The lisfranc ligament is a large oblique ligament that extends from the plantar aspect of the medial cuneiform to the base of the second metatarsal.
The primary stabilizers of the joint include the interosseous ligaments which connect the bases of the 2nd to 5th metatarsals on both the plantar and dorsal aspects. Secondary stabilizers include the plantar fascia, peroneus longus and intrinsic muscles of the foot.
The tarsometatarsal joint complex is divided into four units:
•1st metatarsal: medial cuneiform: 6 degrees mobility.
•2nd metatarsal: middle cuneiform: rigid
•3rd metatarsal: lateral cuneiform: rigid
•4th and 5th metatarsals: cuboid: mobile
The dorsalis pedis artery and the deep peroneal nerve both run between the first and second metatarsal bone.
Mechanism of injury
Direct and indirect mechanisms
•Direct injuries: plantar displacement is more common
•Indirect injuries: more common than direct injuries. Results from axial loading or twisting.
•Dorsal displacement is more common.
Check the alignment of the dorsum of the 2nd metatarsal with the middle cuneiform.
Classification of lisfranc injuries
Lisfranc classifications are not useful in determining the treatment or the prognosis of the injury. Severe injuries are obvious, easily diagnosed and may develop compartment syndrome of the foot. Injuries with minimal displacement could be missed and they will need surgery regardless of the classification. Arthritis may develop even with minimal displacement.
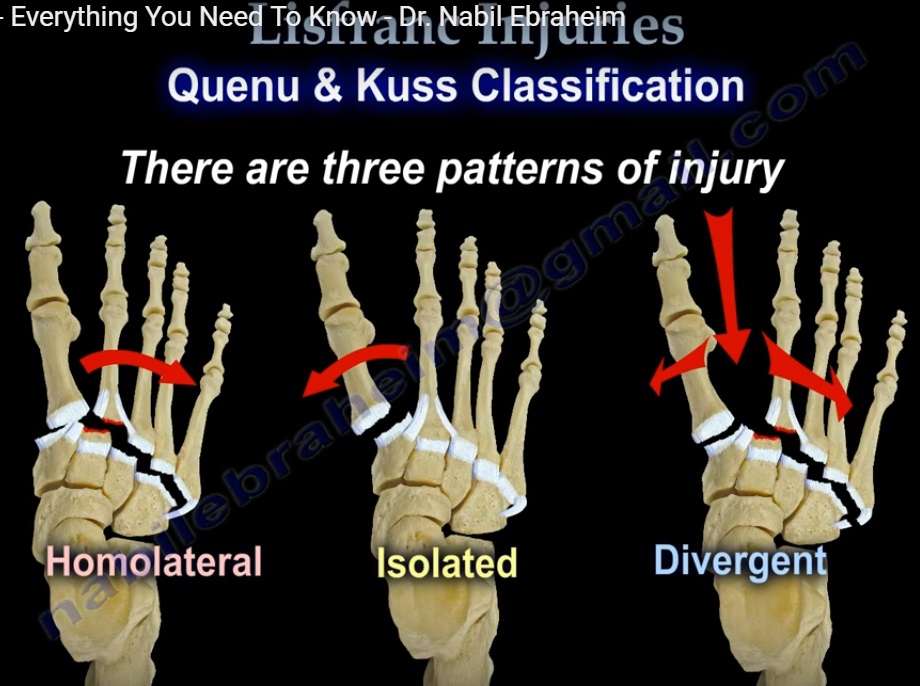
Quenu & Kuss classification
There are three patterns of injury
•Homolateral: all five metatarsals displaced in the same direction.
•Isolated: one or two metatarsals displaced from others
•Divergent: displacement of the metatarsals in both the sagittal and coronal planes.
Hardcastle classification (modification of Quenu & Kuss)
•Homolateral (total incongruity): all five metatarsals displace in common direction. Fracture base of 2nd common.
•Isolated (partial incongruity): displacement of one or more metatarsals away from the others.
•Divergent: lateral displacement of lesser metatarsals with medial displacement of the 1st metatarsals. May have extension of injury into cuneiforms or talonavicular joint.
Myerson classification
Type A (total incongruity)
Type B (partial incongruity) :
•type B1: medial dislocation
•type B2: lateral dislocation
type C (divergent)
•type C1 : partial displacement
•type C2: total displacement
Clinical evaluation
•check the skin condition
•check the neurovascular status
•rule out compartment syndrome
•CT scan is helpful if radiographs are negative
•Prognosis is guarded regardless of the classification
Nice page