Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Elbow Dislocation in Adults
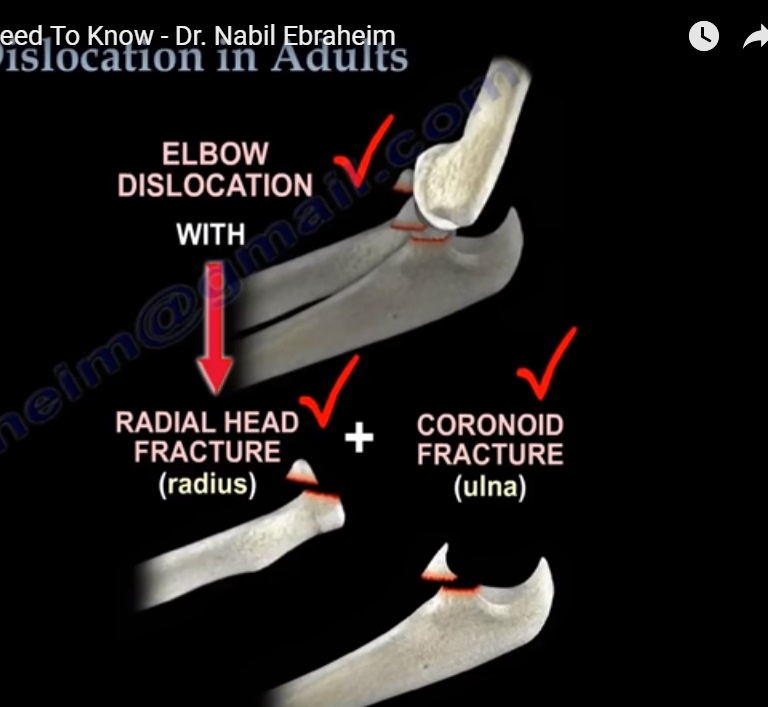
TERRIBLE ELBOW TRIAD
• Elbow dislocation+Radial head fracture+Coronoid fracture of ulna
• The terrible triad is not a simple elbow dislocation, it is a complex elbow dislocation.
• In addition to these three injures of the elbow, there is always a tear of the lateral ulnar collateral ligament.
• The treatment usually is reduction and splinting of the elbow.
• This cannot be the definitive treatment, it is the initial treatment.
• If surgery is not done, chances of recurrent dislocation of the elbow is high
• Surgery is required for reduction and fixation of the fractures and also to restore the elbow stability.
TYPES & CLASSIFICATION
• There are multiple types of elbow dislocation based on the position of the olecranon relative to the humerus.
• The most common type of elbow dislocation is the posterolateral type.
• There are two basic types of elbow dislocations:
1. Simple
- No fracture seen.
- Usually a ligamentous injury
2. Complex
- Associated fractures in addition to the ligamentous injury.
- With any elbow dislocation, one need to check the shoulder and the wrist for injuries and fractures, because it can occur in up to 15%.
- A simple dislocation of the elbow needs a reduction and assessment of stability through the range of motion
- If the elbow is stable with range of motion, then a short period of immobilization with a posterior splint for approximately one week with the elbow in about 90 degrees of flexion is required.
- Recurrence of the dislocation is rare (less than 1%).
- If the elbow is immobilized for more than 3 weeks, there will be severe stiffness of the elbow.
- Surgery is necessary only if it is an irreducible dislocation Or if there is any associated fracture or unable to maintain the stability of the elbow.
TREATMENT OF THE TERRIBLE TRIAD
• Closed reduction (initially).
• Open reduction and internal fixation of the coronoid (if possible), of the radial head or excise the radial head with radial head arthroplasty if the radial head is unreconstructable.
• lateral ulnar collateral ligament repair(LUCL)
ELBOW DISLOCATION WITH OLECRANON FRACTURE
• open reduction and plate fixation of olecranon fracture
• K-wires and tension band is not strong enough to hold the fracture and stabilize the elbow at the same time.
TREATMENT OF ELBOW DISLOCATION WITH RADIAL HEAD FRACTURE
• Do fixation OR replacement of the radial head (excision of the radial head alone in this situation is not acceptable).
LATERAL ULNAR COLLATERAL LIGAMENT
• The LUCL is the most important lesion in recurrence or persistence of instability of the elbow after a simple elbow dislocation.
• The injury progresses from lateral to medial.
• The lateral collateral ligament fails first and it avulses proximally at the lateral epicondyle.
• The medial collateral ligament (MCL) fails last.
VARUS POSTEROMEDIAL ROTATORY INSTABILITY
• In varus posteromedial rotatory instability, there is an elbow injury plus LUCL tear, plus coronoid fracture which involves the medial facet of the coronoid.
CHRONIC DISLOCATION
• Treatment is open reduction, capsular releases with hinge external fixation and early range of motion.
COMPLICATION OF ELBOW DISLOCATION
• Loss of terminal extension.
• Usually for decreased range of motion of the elbow, static progressive splinting is advised for a period of 6-10 weeks.
HETEROTOPIC OSSIFICATION (HO)
• Treatment is excision of Myositis and excise the posterior part of the MCL to allow more flexion.
• To be functional, the range of motion of the elbow should be between 30-130 degrees.
• If the flexion is less than 100 degree, release of the posterior bundle of the MCL in addition to release of the ulnar nerve if needed
• For more flexion of the elbow, excise the posterior part of the MCL also.
Leave a Reply