- Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Anatomy of ligaments of elbow joint - The elbow joint is a hinge joint, formed by the articulation between the lower end of the humerus with the ulna and head of the radius.
- Stability of the elbow joint depends upon the inherent stability of the articulating surfaces, strong capsule and collateral ligaments.
- The Coronoid process is a key stabiliser of the elbow joint and it also the attachment site for the ligament of elbow. It forms the anterior buttress of the olecranon and prevents the posterior dislocation of the elbow.
- Fracture of the coronoid more than 50% of the height will lead to elbow instability.coronoid fracture is often accompanied by anteromedial fracture. The impaction fracture of the anteromedial coronoid facet will lead to posteromedial instability of the joint. These fractures are easily missed in X-rays. Delayed treatment can result in varus and posteromedial instability and osteoarthritis.
- Surgical fixation through a medial approach is the treatment for the same. Fracture of the coronoid process can also be a part of the terrible elbow triad, which includes fracture of coronoid and radial head and elbow dislocation.
The main source of elbow stability is provided by medial and lateral collateral ligament.
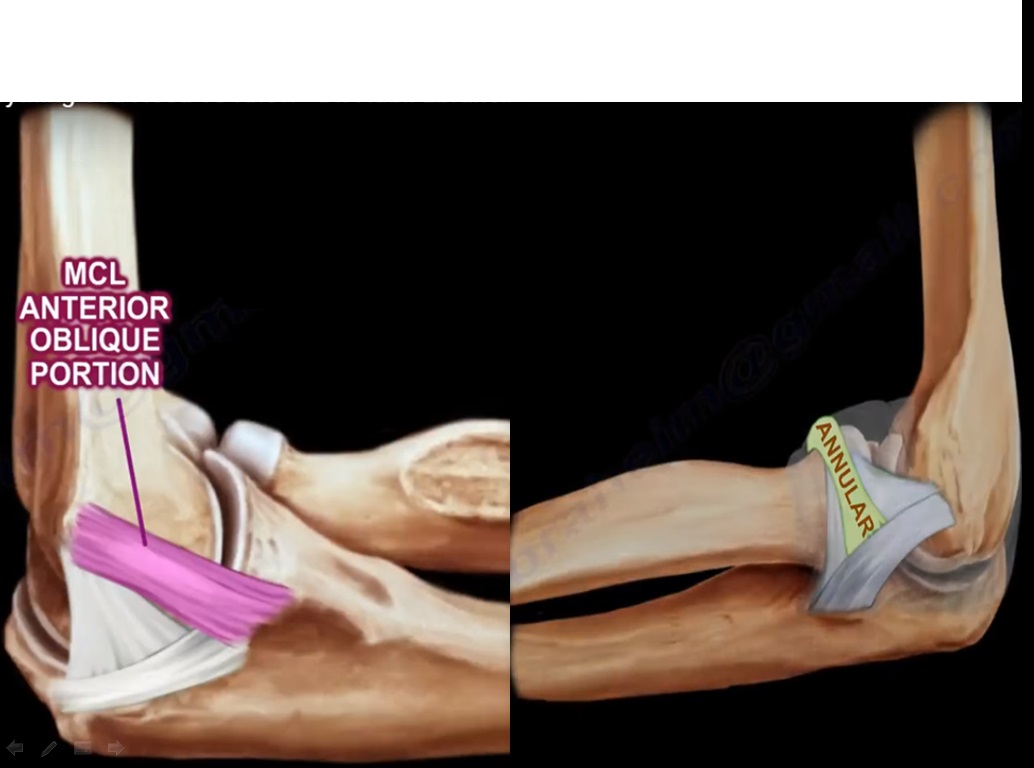
- MCL originates from the posterior medial epicondyle of the distal humerus and inserted into sublime tubercle of the medial coronoid process. It is composed of 3 bands-anterior, posterior and transverse.
- Anterior band of MCL is the strongest primary stabiliser to valgus stress in 90 degree of flexion and in extension it provides about 30 % of the restraint. The posterior portion of MCL forms the floor of the cubical tunnel. The posterior bundle of MCL is tight in elbow flexion. Release of the contracted posterior band of MCL will provide more flexion to the stiff elbow.
- The late cocking and early acceleration will give the highest torque to the MCL. Valgus stress test is used to diagnose MCL deficiency clinically.
- Valgus stress test- with the arm full supinated find the MCL and take the forearm into full extension, placing a valgus stress on MCL.
MRI is the investigation of choice to diagnose complete tear. CT arthrogram is a better option for partial tear.
Treatment-reconstruction of the MCL is the best procedure for complete tears.
Indication for surgery is complete tear in high level throwing athletes which helps in 90 %return to pre injury level of activities.
Lateral collateral ligament
It is composed of 4 parts
1.Lateral ulnar collateral ligament
2.Lateral radial collateral ligament
3.Accessory lateral collateral ligament
4.Annular ligament
- Lateral ulnar collateral ligament is the key anatomic structure which prevents posterolateral instability.
- It originates from the lateral humeral epicondyle and is inserted into crista supinatoris of proximal ulna. It is deep and slightly distal to the common extensor tendon.
- It traverses the posterolateral aspect of the radial head and acts like a sling for the radial head. Posterolateral instability is diagnosed by pivot shift test which comprises of valgus, supination followed by axial compression.
- Surgical approach and arthrotomy to the lateral elbow may damage lateral ulnar collateral ligament resulting in posterolateral instability.
- Iatrogenic injury to the lateral ulnar collateral ligament during surgical correction of tennis elbow and injection of steroid into this area can lead to posterolateral instability.
- It can be a complication of the surgery or can be a part of pathology of the extensor carpi radialis brevis.
- Excessive release of extensor carpi radialis brevis can cause injury to lateral ulnar collateral ligament as it is close to the tendon.
- Patient presents with painful click and difficulty in achieving full elbow extension following surgery. This is better avoided by detaching the tendon and placing it anterior to the equator of the radial head.
Lateral radial collateral ligament and accessory lateral collateral ligament has some contribution to lateral elbow stability.
Annular ligament stabilises the radio ulnar joint.
Secondary static stabilisers-Radial head provides approximately 30 % of the valgus stability.
Leave a Reply