Cobalt poisoning by hip replacement: Arthroprosthetic-Cobaltism
Stephen Tower, MD, University of Alaska, Alaska, USA
- Cobalt, in excess, has the potential to block oxidative metabolism at the mitochondrial level.
- The peripheral and central nervous systems, the heart, and the thyroid gland are variably compromised whether the means of cobalt exposure is iatrogenic (use of cobalt chloride as a hematemic), industrial (exhalation or ingestion of cobalt powders or ores), from the ingestion of cobalt laced beer (beer drinkers cardiomyopathy), or arthroprosthetic (wear of chrome-cobalt articular surfaces or corrosion and fretting of modular chrome-cobalt femoral necks and heads).
- The toxicity of cobalt has been known since 1948.(1 2)
- The first case report of arthroprosthetic-cobaltism was in Italian in 2001. The mechanism was wear or a revision chrome-cobalt femoral head by ceramic bits from the primary fractured ceramic component embedded in the revision plastic socket liner.
- The degree of hypercobaltemia was unreported; symptoms of peripheral neuropathy were first noted 9 months after the first revision operation. Diagnosis was serendipitous.
- A metal laden pericardial effusion was found on CT scan, prompting a radiograph of the asymptomatic hip revealing an aspherical femoral head. Resection arthroplasty was not performed until 16 months after the first revision operation, by then the patient’s pathology had progressed to severe motor and sensory neuropathy, pericardial tamponade, and hypothyroidism(.3)
- Reports of 8 additional extreme cases of cobaltism from the ceramic-on-metal wear have followed. Blood cobalt levels in mcg/L ([BCo]) have ranged from 400 to 1000, latency to symptoms ranged from 3-48 months, and latency to diagnosis or revision surgery from 9 to 72 months.
- All patients had neurologic pathology, most were hypothyroid, and all but three were noted to have cardiomyopathies. One patient died of heart failure, those patients followed > 6 months post second revision improved as their [BCo] declined.
- The typical presentation of cobaltism was fatigue and anorexia, followed by numbness and weakness, hypothyroidism, deafness and blindness, and finally and sometimes fatally, heart failure or arrhythmias. Hypothyroidism was diagnosed in most cases before the diagnosis of cobaltism was made and some clinical improvement noted with onset of thyroid replacement therapy. None of the patients had notable sentinel hip symptoms before onset of overt systemic pathology.(4-11)
The mean [BCo] of the general population is 0.2 mcg/L and a level of > 1 mcg/L raises concern of excessive industrial cobalt exposure(.12)Long term, low grade, vocational cobalt exposure has been linked to echocardiographic cardiomyopathy and subtle neurocognitive defects.(13,14) Patients with tribolically well functioning metal-on-metal hip resurfacings and a median [BCo] of 1.6 mcg/L had echocardiographic cardiomyopathy compared to matched controls with metal-on-plastic hips with a median [BCo] of < 0.3 mcg/L.(15 )Patients with steep or excessively anteverted BHR (Smith and Nephew) resurfacings or patients with ASR (DePuy) stemmed and resurfacing components frequently have [BCo] > 10.(16,17)
- The first case reports of cobaltism from articular surface wear of contemporary metal-on-metal hips were published out of Alaska in 2010.18
- Both men were implanted with ASR XL (DePuy) stemmed metal-on-metal hips and manifested progressive illnesses with a latency of a year including: fatigue, disorder sleep and mood, audio-vestibular pathology, and symptomatic cardiomyopathy with improvement after the ASR hips were explanted after 42 months in situ. [BCo] s of 23 and 122 were noted and the patient with the worst manifestations had the highest [BCo].
- The JBJS report of these cases was meet with measured skepticism by the Presidential Line of the AAOS.19,20
After the JBJS case report cobaltism from contemporary metal-on-metal stemmed and resurfacing hips is reported with increasing frequency noting a similar syndrome, latency, reversibility, and [BCo] s as the Alaskan index cases.21-26
- Neurologic symptomatology is common to most Arthroprosthetic Cobaltism case reports and the severity of neurologic manifestations can be quantitated (Table 1).
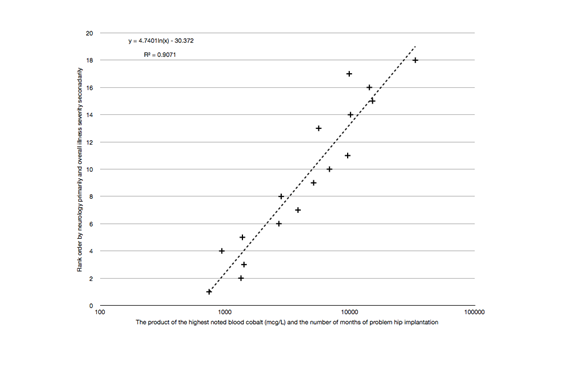
- The rank order of the Arthroprosthetic Cobaltism cases by the severity of neurologic symptoms and general illness severity (Table 2) appears to be a function of the product of the months of hip implantation and the highest noted [BCo] before revision surgery (Figure 1).
Table 1: Grading Scheme for Cardiac and Neurologic Cobaltism Manifestations
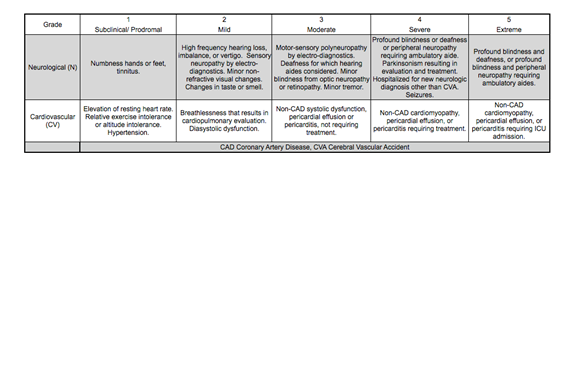
Table 2: Case Reports of Arthroprosthetic Cobaltism rank ordered primarily by severity of neurologic Manifestations.
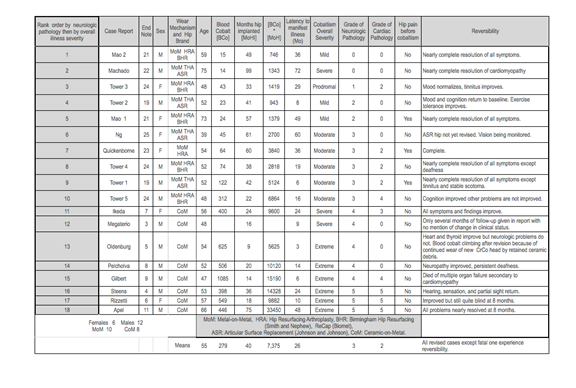
Figure 1: Plot of rank order of Arthroprosthetic Cobaltism Cases primarily by neurologic severity to the product of months of hip implantation and [BCo]
- A cross-sectional cohort study will be required to determine the incidence and prevalence of hypercobaltemia, cobaltism, and pseudotumors among patients implanted with metal-on-metal hips.
- A study of Dutch patients implanted with BHRs noted that most patients at 8 years post implantation were hypercobaltemic and had pseudotumors by CT scan; the patients were not surveyed for the manifestations of cobaltism.27
- The surgeons of the author’s clinic have now revised 33 metal-on-metal hips, median pre-revision [BCo] was > 40, and a third of the patients developed constitutional, neurologic, or cardiac manifestations consistent with cobaltism that resolved after revision to a ceramic-on-plastic articulation and decline of [BCo].
- The Alaskan and the Dutch experience suggest that hypercobaltemia, pseudotumors, and cobaltism are likely common in patients implanted with contemporary metal-on-metal hips for > 5 years.
Until recently reported cases of cobaltism related to contemporary stemmed and resurfacing metal-on-metal hips have featured lower [BCo] and a less severe illness than those cases resulting from ceramic-on-metal wear. An overlap case was just reported in NEJM, the 59 year-old female was implanted with bilateral ASR hips for 4 years then required heart transplantation for cardiomyopathy. A prodrome of fatigue was reported but neurologic manifestations were not reported. The diagnosis of cardiac cobaltism was not made until a year post heart transplantation when the function of the graft was declining and [BCo] of 288 was noted. The graft recovered and the patient’s fatigue resolved after revision of the ASR hips and a decline in [BCo].28
- The most popularized case of arthroprosthetic cobaltism just appeared in Lancet. The diagnosing physician recognized of the syndrome from an episode of “House” in which Cuddy’s mother (played by Candace Bergman) was found to have arthroprosthetic cobaltism by Dr. House after exhibiting a focal neurologic finding (inability to recognize sarcasm) and progressive cardiomyopathy.
- The male German patient of the Lancet case report was deaf, blind, hypothyroid, and was pending heart transplantation. He became symptomatic 6 months after revision of a fractured ceramic implant to metal-on-plastic hip implants, a [BCo] of 904 was noted and second revision not performed until 32 months after the first revision.
- The patient’s cardiomyopathy resolved after second revision but he continues to have significant deafness and blindness.10
- Patients with chrome-cobalt implants with modular junctions can also be hypercobaltemic and manifest periprosthetic pseudotumors.29 The Rejuvenate stem (Stryker) that features a supernumerary junction between a chrome-cobalt neck and a titanium stem is particularly problematic and has been recalled from the market.30
- We are not aware of a published cast report of cobaltism resulting from taper generated chrome-cobalt metallosis but we have identified several Alaskan patients with “double digit” hypercobaltemia from their Rejuvenate stems with cobaltism manifestations that resolved after revision of the Rejuvenate stem to a Monoblock titanium stem with a ceramic head.
The Alaskan experience indicates that hypercobaltemia and cobaltism are epidemic in patients with metal-on-metal hips and endemic in patients with the recalled Stryker Rejuvenate stems.
- Prodromal cobaltism consists of non-specific constitutional symptoms: fatigue, disordered sleep and mood, and anorexia. Clinical neurologic manifestations are generally progressive: audio-vestibular, then peripheral neuropathic, followed by blindness.
- Diastolic dysfunction as been common to all Alaskan cobaltism cases in which echocardiography was performed. Echocardiography may be a quantitive means of following hypercobaltemic patients for early toxicity.
- Systematic annual surveillance of patients implanted with metal-on-metal hips (stemmed and resurfacing) and Rejuvenate stems with [BCo] and review by the surgeon for pseudotumors and by the primary medical provider for cobaltism is mandated.31
- Revision surgery should be considered for patients with significant pseudotumors, “double digit” cobaltemia, and for hypercobaltemic patients with progressive systemic manifestations consistent with cobaltism.32 We recommend revision to a titanium stem and a ceramic-on-plastic articulation.
Ref:
1. Tower S. Arthroprosthetic cobaltism: identification of the at-risk patient. Alaska Med. Sep 2010;52:28-32.
2. Smith IC, Carson BL. Volume 6-Cobalt An Apraisal of Environmental Exposure. 1st ed. Ann Arbor: Ann Arbor Science; 1981.
3. Megaterio S GF, Alossa E, Capretto S. Effetti a distanza del rilascio di ioni metallo in usura della testa protesica:
presentazione di un caso. G.I.O.T. 7/2/01 2001;27:173-175.
4. Steens W, von Foerster G, Katzer A. Severe cobalt poisoning with loss of sight after ceramic-metal pairing in a hip–a case report. Acta Orthop. Oct 2006;77(5):830-832.
5. Oldenburg M, Wegner R, Baur X. Severe cobalt intoxication due to prosthesis wear in repeated total hip arthroplasty. J Arthroplasty. Aug 2009;24(5):825 e815-820.
6. Rizzetti MC, Liberini P, Zarattini G, et al. Loss of sight and sound. Could it be the hip? Lancet. Mar 21 2009;373(9668):1052.
7. Ikeda T, Takahashi K, Kabata T, Sakagoshi D, Tomita K, Yamada M. Polyneuropathy caused by cobalt-chromium metallosis after total hip replacement. Muscle Nerve. Jul 2010;42(1):140-143.
8. Pelclova D, Sklensky M, Janicek P, Lach K. Severe cobalt intoxication following hip replacement revision: Clinical features and outcome. Clin Toxicol (Phila). Apr 2012;50(4):262-265.
9. Gilbert CJ, Cheung A, Butany J, et al. Hip Pain and Heart Failure: The Missing Link. The Canadian journal of cardiology. Jan 8 2013.
10. Dahms K, Sharkova Y, Heitland P, Pankuweit S, Schaefer JR. Cobalt intoxication diagnosed with the help of Dr House. The Lancet. 2014;383(9916):574.
11. Apel W, Stark D, O’Hagan S. An update on cobalt-chromium toxic retinopathy. Doc Ophthalmol. May 10 2013.
12. Catalani S, Rizzetti MC, Padovani A, Apostoli P. Neurotoxicity of cobalt. Hum Exp Toxicol. Jul 5 2011.
13. Linna A, Oksa P, Groundstroem K, et al. Exposure to cobalt in the production of cobalt and cobalt compounds and its effect on the heart. Occup Environ Med. Nov 2004;61(11):877-885.
14. Jordan CM, Whitman RD, Harbut M. Memory deficits and industrial toxicant exposure: a comparative study of hard metal, solvent and asbestos workers. Int J Neurosci. Jun 1997;90(1-2):113-128.
15. Prentice JR, Clark MJ, Hoggard N, et al. Metal-on-Metal Hip Prostheses and Systemic Health: A Cross-Sectional Association Study 8 Years after Implantation. PloS one. 2013;8(6):e66186.
16. De Haan R, Pattyn C, Gill HS, Murray DW, Campbell PA, De Smet K. Correlation between inclination of the acetabular component and metal ion levels in metal-on-metal hip resurfacing replacement. J Bone Joint Surg Br. Oct 2008;90(10):1291-1297.
17. Langton DJ, Joyce TJ, Jameson SS, et al. Adverse reaction to metal debris following hip resurfacing: the influence of component type, orientation and volumetric wear. J Bone Joint Surg Br. Feb 2011;93(2):164-171.
18. Epidemiology A. Cobalt Toxicity in Two Hip Replacement Patients. State of Alaska Epidemiology Bulletin. May 28, 2010 2010(Bulletin No. 14).
19. Tower SS. Arthroprosthetic cobaltism: neurological and cardiac manifestations in two patients with metal-on-metal arthroplasty: a case report. J Bone Joint Surg Am. Dec 1 2010;92(17):2847-2851.
20. Jacobs JJ. Commentary on an article by Stephen S. Tower, MD: “Arthroprosthetic cobaltism: neurological and cardiac manifestations in two patients with metal-on-metal arthroplasty. a case report”. J Bone Joint Surg Am. Dec 1 2010;92(17):e35.
21. Mao X, Wong AA, Crawford RW. Cobalt toxicity – an emerging clinical problem in patients with metal-on-metal hip prostheses? Med J Aust. Jun 20 2011;194(12):649-651.
22. Machado C, Appelbe A, Wood R. Arthroprosthetic Cobaltism and Cardiomyopathy. Heart, lung & circulation. Apr 18 2012.
23. Van Der Straeten C, Van Quickenborne D, DeSmet K. Hearing loss in a bilateral hip resurfacing. Tijdschr. voor Geneeskunde. 1/2012
2012;68(00).
24. Tower SS. Arthroprosthetic cobaltism associated with metal on metal hip implants. Bmj. 2012;344:e430.
25. Ng SK, Ebneter A, Gilhotra JS. Hip-implant related chorio-retinal cobalt toxicity. Indian journal of ophthalmology. 2013;61(1):35.
26. Van Der Straeten C. Further cases of arthroprosthetic cobaltism from Gent. Personal Communication. 9/2/2013 2013.
27. Holland JP, Langton DJ, Hashmi M. Ten-year clinical, radiological and metal ion analysis of the Birmingham Hip Resurfacing: from a single, non-designer surgeon. J Bone Joint Surg Br. Apr 2012;94(4):471-476.
28. Allen LA, Ambardekar AV, Devaraj KM, Maleszewski JJ, Wolfel EE. Clinical problem-solving. Missing elements of the history. The New England journal of medicine. Feb 6 2014;370(6):559-566.
29. John Cooper H. Corrosion at the Head-Neck Taper as a Cause for Adverse Local Tissue Reactions After Total Hip Arthroplasty. The Journal of Bone and Joint Surgery (American). 2012;94(18):1655.
30. Pivec R, Meneghini RM, Hozack WJ, Westrich GH, Mont MA. Modular Taper Junction Corrosion and Failure: How to Approach a Recalled Total Hip Arthroplasty Implant. J Arthroplasty. 2014;29(1):1-6.
31. MEDICINEWISE N. Monitoring for potential toxicity in patients with metal-on-metal hip prostheses: advice for health professionals. 2013.
32. Kwon Y-M, Lombardi AV, Jacobs JJ, Fehring TK, Lewis CG, Cabanela ME. Risk Stratification Algorithm for Management of Patients with Metal-on-Metal Hip ArthroplastyConsensus Statement of the American Association of Hip and Knee Surgeons, the American Academy of Orthopaedic Surgeons, and The Hip Society. The Journal of Bone & Joint Surgery. 2014;96(1):e4-6.
Leave a Reply