Management of Aseptic nonunion of tibia
Aetiology: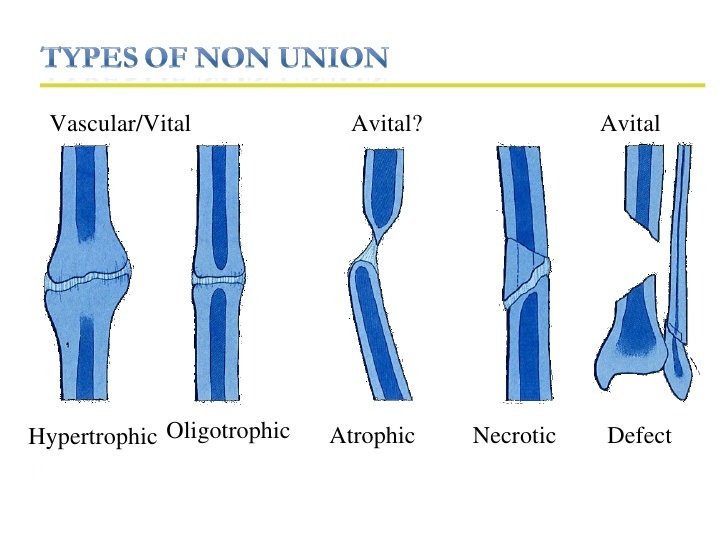
- Nonunion following fracture tibia is a common orthopaedic problem. The presence of infection and bone loss will complicate the management of these fractures
- Soft tissue damage and periosteal stripping are common in high velocity and open injuries and this can compromise the vascularity to the soft tissues around the fracture
- Surgical technique, internal fixation methods, placement of the fracture in distraction can lead to further disruption of normal fracture healing.
- Hypertrophic nonunion can be caused by excessive movement at the fracture site.
- Nicotine usage and NSAIDs have a negative influence on fracture healing.(1)
- Bhandari and colleagues identified risk factors for nonunion as presence of an open fracture, presence of postoperative fracture gap,transverse fracture and more distal location of a tibia fracture(26, 27)
Diagnosis:
- Several arbitrary time points have been given to designate tibial nounion, with ranges from 20 to 26 months(2)
- FDA had defined nonunion as absence of radiographic healing 9 months after injury
- Absence of progressive signs of healing on radiographs for 3 consecutive months has been suggested as a newer definition so that the nonunion can be intervened early and prolonged morbidity can be avoided.
- Pain on weight bearing is a classical symptom of nonunion
- Palpable motion maybe present, but can be obscured in the presence of fibrous nonunion.
- CT has been suggested as a method to detect nonunions when radiographs are inconclusive. CT scan is highly sensitive, but specificity has been poor as healed fractures have been mistaken as nonunions in CT(3)
- The traditional classification of Weber and Cech have been used widely. They had classified Nonunions as hypertrophic and atrophic nonunions(4)
- The authors believed that atrophic nonunions were avascular and required a biologic stimulus to promote healing.
- Recent studies have questioned the philosophy that all atrophic nonunions are avascular(5)
Principles of Management
- Occult infection should be rule out, especially if the fracture was an open injury earlier
- WBC counts may not be particularly useful, but ESR and CRP maybe of use.
- MRI can detect bone marrow changes consistent with infection, but presence of metal artifacts and postoperative changes can interfere with interpretation of the sequences
- Indium labeled WBC scan also an be used to diagnose underlying bone infection; but false positive result may occur in patients with an unstable nonunion and in those with a periarticular nonunion with associated arthritic changes
- Nonsurgical management can be considered in patients with well aligned, stable tibial nonunions, particularly in those who are considered poor surgical candidates due to medical comorbidities or impaired soft tissue.
- A careful step-by-step surgical plan with a detailed drawing of planned deformity correction and final fixation is useful for surgical management of tibial nonunion.
- Preoperative antibiotics are withheld until the results of culture and sensitivity patterns of deep infection are obtained.
- Hypertrophic nonunion is managed by stable fixation and axial compression or lag screw fixation.
- Atrophic nonunions are managed by adding a biologic stimulus like bone graft
- Sagittal, coronal and rotational planes need to be analyzed for deformity correction
- New screws maybe difficult to be applied due to presence of previous screw holes and subsequent lysis.
- A local rotational flap or free-flap coverage may be required in the setting of a tenuous soft-tissue envelope with prior surgical scars and adherent nonmobile skin
Extracorporeal Shock Wave Therapy
- Basic science studies have shown increased bone mass and strength, angiogenesis, and differentiation of mesenchymal stem cells. A recent study be Caccio et al..found it to be useful for hypertrophic nonunions
Low Intensity Pulsed Ultrasound
- Low-intensity pulsed ultrasound (LIPUS) involves transcutaneous transmission of mechanical energy in the form of high-frequency acoustical pressure waves to the site of nonunion
- Daily LIPUS treatment for as little as 20 minutes is effective in stimulating healing.
- Currently no Level I study is available to justify the use of LIPUS in tibial nonunions
Electrical Stimulation
- Only 4 randomized studies have been conducted in the past comparing fracture healing with PEMF(Pulsed Electromagentic field)and without PEMF
- The most recent level I study by Sam Adie et al..in tibial nonunions found no difference in patients treated with PEMF and controls where PEMF was not used
Functional Cast Bracing
- functional bracing combined with fibular osteotomy is an option in the patient with a stable nonunion and sufficient healing potential(7)
SURGICAL MANAGEMENT
- Options for nonunion following prior intramedullary (IM) nailing, including exchange reamed nailing, adjunctive plate fixation, conversion to plate fixation, and external fixation
- Conversion to an external fixator is typical for the management of infected non union of the tibia
Exchange Reamed Nailing
- Exchange reamed nailing improved mechanical stability in patients with diaphyseal nonunion because the larger diameter IM nail has increased endosteal contact
- Exchange reamed nailing will not improve mechanical stability in patients with metadiaphyseal nonunions; hence, other options like plate fixation should be considered
- Two beneficial effects of reaming are: increased periosteal blood flow and stimulation of periosteal bone formation
- Compression of nonunion can be achieved by reverse impaction or by using a nail with internal compression systems. This can be achieved by performing distal locking initially and then placing a dynamic locking screw proximally and then an internal locking screw is advanced against the proximal locking screw to achieve compression at the fracture site.
- Fibular osteotomy does not need to be routinely performed; occasionally it may be needed for deformity correction.
- Success rates from 75% to 100% have been achieved for reamed exchange nailing(8)
- Reamed exchange nailing is contraindicated in the presence of infection.
Adjunctive plate fixation
- Advocates of adjunctive plate fixation with a nail in situ argue that, there would be some residual motion after a statically locked IM nail. This can be reduced by plate fixation
- This is especially suited for patients with hypertrophic nonunions to provide additional stability
- And also useful in patients with metaphyseal nonunions, where a large diameter nail alone may not have sufficient endosteal contact to provide absolute stability(Ueng SW et al-9)
Nail Removal and Plating
- This can be useful for metaphyseal nonunions where nails will not provide sufficient endosteal contact.
- Compression can be achieved using interfragmentary lag screws, dynamic compression plates and external compression devices(10)
- But plate fixation is associated with possibility of soft tissue devascularisation due to need for obtaining proper exposure
External fixation using Ilizarov Method:
- This is a versatile management system which can be used for deformity correction, nonunion compression, an distraction osteogenesis of bone defects and correction of limb length discrepancy.
- Useful to treat infected nonunions that have been managed with radical resection of the infected bone and distraction osteogenesis
- Allows full weight bearing and even useful for patients over 60 years.
Internal Fixation
- blade plates offer improved fixation compared with standard compression plates in short segments of bone
- the 90° cannulated blade plate can be placed medially, posteriorly, or laterally in distal tibial nonunions
- Soft-tissue condition and prior surgical approaches may dictate optimal plate position.
- Locking plates have been useful for the management of humeral nonunions and short bone segments.
- Revision ORIF with plating is best indicated for tibial nonunion in the metaphyseal region of the proximal or distal tibia
- Compression of fracture site should be achieved using interfragmentary screw or axial compression
- Axial compression can be done using dynamic holes in a compression plate or a external compression device like the Muller’s compression device
- Bone healing typically begins along the posterior and lateral borders of the tibia where the muscle attachment provides good vascularity
- Plate placement along the subcutaneous anteromedial tibial border avoids posterior and lateral periosteal disruption
- Placement of the plate along the posterior border of the tibia requires additional surgical dissection but is useful in managing tibial nonunion in the distal one half of the tibia.
- A posterolateral bone graft can be placed through the same surgical approach.
- Some surgeons advocate extensive takedown of the nonunion with removal of the intervening fibrous tissue. Alternatively, the fibrous tissue can be left in place and rigid compression applied to the nonunion.
- The adjacent bone cortex also can be petaled or shingled with an osteotome to increase the surface area of the bone and stimulate additional healing response.
Partial Fibulectomy
- Partial fibulectomy with application of PTB cast has been used historically to treat tibial nonunion
- To avoid tibial destabilization, the fibulectomy should be performed at a site other than that of the nonunion.(11)
- Fibulectomy may be needed to correct deformity.
Dynamisation
- Level 1 studies are lacking regarding the role of dynamisation in the healing of diaphyseal fractures. Court Brown and colleagues suggested that dynamisation has no role in fracture healing.(18)
Bone Graft and Bone Graft Alternatives
- Autologous bone graft is osteogenic, osteoinductive, and osteoconductive properties
- A posterolateral approach is typically used for placement of bone graft in tibial nonunions. This approach offers the advantage of avoiding the subcutaneous anterior border of the tibia, which is often compromised by prior open injury or surgical incision.
- In addition, the improved vascular supply provided by the posterior muscles is believed to enhance graft incorporation
- Masquelet and Begue popularized the placement of a temporary cement spacer into segmental bone defects to form a reactive membrane. (12)
- Basic science studies have shown that this induced membrane secretes various growth factors that may be beneficial for subsequent bone graft incorporation(19)
Bone defects:
- Bone defects can be classified as OTA class I is there is loss of 50% of circumference of bone. Type2 if there is loss of more than 50% of circumference of bone or type 3 if there is a missing bone segment(20)
- Type 1 bone defects and fracture with less than 2 cm defects can be managed with reamed exchanged nailing. (Court Brown et al..15)
- Type 2 bone defects and fractures with gaps of 2-6 cm require additional bone grafts or bone graft substitutes in addition to reamed exchange nailing(16)
- Fractures with more than 6 cm bone defect require, individualized treatment. This include Ilizarov external fixator and bone transport, vascularised fibular graft and lengthening over a nail(17)
- Ilizarov external fixator is a versatile system, whereby large defects can be reconstructed.
- Vascularised fibular grafts have been used successfully to treat large defects. This procedure requires considerable technical expertise and it is technically challenging
- Lengthening can also be performed using a monorail system and performing segmental transport
Bone Graft Harvest
- Reamer-Irrigator-Aspirator (RIA, Synthes, West Chester, PA) was initially designed to decrease embolic complications, but has been successfully used to obtain huge amounts of bone graft

- Segmental defects have been bridged with bone grafts harvested from RIA. Also, Belthur et al..reported improved pain scores at the hip compared to Iliac crest bone grafting(13,14)
Bone Marrow Aspiration and Injection
- Level IV studies are available for the use of Bone Marrow Aspiration and Injection for the treatment of tibial nonunions
- A potential limitation of this treatment is the variability of osteoprogenitor cells among patients and the decrease in these cells that occurs with aging(21)
Stem cells
- Stem cells can be harvested, expanded and implanted into the fracture site to promote union
- A high rate of healing was reported in a commercial study in which tibial nonunions were managed with cultured autologous bone marrow stem cells, but the study has not been published till date(Jimenez ML,-22)
Bone Morphogenic Proteins
- Friendlander in a level I study found beneficial effects for the use of rh-BMP 7 for the use of tibial nonunion when compared with iliac crest bone grafting(23)
- US FDA as still not approved the use of rhBMP-7 for the use of tibial nonunion, since reamed nailings were used in 90% of patients in Friedlander’s study and it is unknown whether reamed nailings were a stimulus for fracture healing in the study.
- Union rate of 100% was obtained in a level IV study (Giannoudis PV et al..) comprising 45 nonunions(16 tibial nonunions) in which rhBMP-7 was combined with iliac crest bone grafting. The authors postulated beneficial effect of rhBMP-7 when combined with Iliac crest bone grafting(24)
- Similarly, off label use of rhBMP-2 is common in the United States, though there is lack of clinical evidence for its beneficial effect in nonunions. rh-BMP2 has been approved by the US FDA for use in acute open fractures of the tibia(25)
References
- Kwong FN, Harris MB: Recent developments in the biology of fracture repair. J Am Acad Orthop Surg 2008; 16(11):619-625.
- Pheifer LS, Goulet JA: Delayed unions of the tibia. J Bone Joint Surg 2006;88(1): 206-216.
- Bhattacharyya T, Bouchard KA, Phadke A, Meigs JB, Kassarjian A, Salamipour H: The accuracy of computed tomography for the diagnosis of tibial nonunion. J Bone Joint Surg Am 2006; 88(4):692-697.
- Weber BG, Cech O: Pseudarthrosis: Pathology, Biomechanics, Therapy, Results. Berne, Switzerland, Hans Huber Medical Publisher, 1976.
- Reed AA, Joyner CJ, Brownlow HC, Simpson AH: Human atrophic fracture non-unions are not avascular. J Orthop Res 2002;20(3):593-599.
- Cacchio A, J Bone Joint Surg Am 2009;91(11)
- Sarmiento A, Burkhalter WE, Latta LL: Functional bracing in the treatment of delayed union and nonunion of the tibia. Int Orthop 2003;27(1):26-29.
- Brinker MR, O’Connor DP: Exchange nailing of ununited fractures. J Bone Joint Surg Am 2007;89(1):177-188.
- Ueng SW, Liu HT, Wang IC: Augmentation plate fixation for the management of tibial nonunion after intramedullary nailing. J Trauma 2002; 53(3):588-592.
- Rodriguez-Merchan EC, Gomez-Castresana F: Internal fixation of nonunions. Clin Orthop Relat Res 2004;
- Connolly JF: Common avoidable problems in nonunions. Clin Orthop Relat Res 1985;(194):226-235.
- Masquelet AC, Begue T: The concept of induced membrane for reconstruction of long bone defects. Orthop Clin North Am 2010;41(1):27-37.
- McCall TA, Brokaw DS, Jelen BA, et al:Treatment of large segmental bone defects with reamer-irrigator-aspirator bone graft: Technique and case series. Orthop Clin North Am 2010;41(1):63- 73.
- Belthur MV, Conway JD, Jindal G, Ranade A, Herzenberg JE: Bone graft harvest using a new intramedullary system. Clin Orthop Relat Res 2008; 466(12):2973-2980.
- Court-Brown CM, Keating JF, Christie J, et al. Exchange intramedullary nailing. Its use in aseptic tibial nonunion. J Bone Joint Surg Br 1995;77(3):407-411
- Keating JF, Simpson AH, Robinson CM. The management of fractures with bone loss. J Bone Joint Surg Br 2005;87(2):142-150.
- Dagher F, Roukoz S. Compound tibial fractures with bone loss treated by the Ilizarov technique. J Bone Joint Surg Br 1991;73(2):316-321.
- Court-Brown CM, Christie J, McQueen MM. Closed intramedullary tibial nailing. Its use in closed and type I open fractures. J Bone Joint Surg Br 1990;72(4):605-611.
- Pelissier P, Masquelet AC, Bareille R, Pelissier SM, Amedee J: Induced membranes secrete growth factors including vascular and osteoinductive factors and could stimulate bone regeneration. J Orthop Res 2004;22(1): 73-79.
- Court-Brown CM. Fractures of the Tibia and fibula. In: Bucholz R, Heckman J, Court-Brown C, et al, eds. Rockwood and Green’s Fractures in Adults, 6th ed. Philadelphia, PA: Lippincott Williams and Wilkins, 2005:2079-2146
- Muschler GF, Boehm C, Easley K: Aspiration to obtain osteoblast mprogenitor cells from human bone marrow: The influence of aspiration volume. J Bone Joint Surg Am 1997; 79(11):1699-1709.
- Jimenez ML, Lyon T, Nowinski G, et al: Abstract: High-dose stem and progenitor cell therapy for refractory long-bone nonunions: Final Results of a multicenter phase I/II clinical study. Presented at the 2007 meeting of the Orthopaedic Trauma Association, Boston, MA, October 17-18, 2007. Available at: http://www.hwbf.org/ota/am/ota07/ otapa/OTA070317.htm. Accessed July 11, 2011.
- Friedlaender GE, Perry CR, Cole JD, et al: Osteogenic protein-1 (bone morphogenetic protein-7) in the treatment of tibial nonunions. J Bone Joint Surg Am 2001;83(pt 2 suppl 1): S151-S158.
- Giannoudis PV, Kanakaris NK,Dimitriou R, Gill I, Kolimarala V, Montgomery RJ: The synergistic effect of autograft and BMP-7 in the treatment of atrophic nonunions. Clin Orthop Relat Res 2009;467(12):3239-3248.
- Dahabreh Z, Calori GM, Kanakaris NK,Nikolaou VS, Giannoudis PV: A cost analysis of treatment of tibial fracture nonunion by bone grafting or bone morphogenetic protein-7. Int Orthop 2009;33(5):1407-1414.
- Audige L, Griffin D, Bhandari M, et al. Path analysis of factors for delayed healing and nonunion in 416 operatively treated tibial shaft fractures. Clin Orthop Relat Res 2005; 438:221-232.
- Bhandari M, Tornetta P III, Sprague S, et al. Predictors of reoperation following operative management of fractures of the tibial shaft. J Orthop Trauma 2003;17(5):353-361.
Leave a Reply